 |
Research Article
Challenges and outcome of management of breast cancer in Abakaliki, South East Nigeria
1 Fellow West African College of Surgeons, FWACS (Consultant Surgeon), Department of Surgery, Alex Ekwueme Federal University Teaching Hospital, Abakaliki, Ebonyi State, Nigeria
2 Fellow National Postgraduate Medical College of Nigeria, FMCS (Consultant Surgeon), Department of Surgery, Alex Ekwueme Federal University Teaching Hospital, Abakaliki, Ebonyi State, Nigeria
Address correspondence to:
Uche Emmanuel Eni
Department of Surgery, Alex Ekwueme Federal University Teaching Hospital (AE-FUTH), Abakaliki, Ebonyi State,
Nigeria
Message to Corresponding Author
Article ID: 100009C01UE2019
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Eni UE, Dilibe UC, Ugwu OA, Daniel UHA, Onyeyirichi O, Ekuma OU. Challenges and outcome of management of breast cancer in Abakaliki, South East Nigeria. Edorium J Cancer 2019;5:100009C01UE2019.ABSTRACT
Aims: Though the incidence of breast cancer is apparently higher in the developed world than in developing countries, the mortality rate is known to be much higher among African women. The paradox has been attributed to a myriad of factors including late presentation with advanced disease and unfavorable biologic subtypes. The aim of this study is to highlight the challenges that are peculiar to our practice in breast cancer management in Abakaliki, South East Nigeria.
Methods: This was a prospective study of all patients diagnosed with breast cancer seen in a general surgery unit at Federal Teaching Hospital, Abakaliki between January 2014 and April 2016. Data obtained from patients’ folders complemented by oral interview during follow-up visits in the clinic or ward admission were entered in a pro forma and analyzed.
Results: A total of 89 patients with histological diagnosis of breast cancer were studied. The mean age was 45.8 (±11.7) years. Fifty patients (56.2%) were premenopausal. The vast majority (79.8%) of patients presented with advanced disease, many (33.6%) with fungation. Diagnosis was essentially by histology, in the absence of facility for immunohistochemistry. Staging investigations were basically chest X-ray, abdominal ultrasound scan, and plain bone X-rays. Treatment options were mostly limited to surgery, chemotherapy, and hormonal therapy, due to unavailability of radiotherapy and monoclonal antibody/other targeted therapy. Recurrence was therefore common and posed a serious challenge in the management of breast cancer in our setting. Outcome was therefore generally poor.
Conclusion: Breast cancer is common in our practice and often present late. Increased awareness, poverty alleviation, and organized screening program are necessary to reduce late presentation and improve prognosis.
Keywords: Abakaliki, Breast cancer, Challenges, Management
INTRODUCTION
Breast cancer is a common presentation in our practice [1]. It is currently the most common cancer in women worldwide, with rising incidence in hitherto low risk countries of Asia and Sub-Saharan Africa [2],[3],[4]. However, a worldwide variation in the incidence and mortality from the disease is well documented [5],[6]. Though the incidence of breast cancer is higher in the developed world than in the developing countries, the mortality rate is reported to be significantly higher among African women [7],[8]. This paradox has been attributed to a number of factors including late presentation with advanced disease and unfavorable biologic subtypes [7],[9]. Late presentation is attributed to ignorance, poverty, fear of the unknown, believe in alternative medicine, lack of confidence in orthodox medicine, and limited access to appropriate health care facility [10],[11]. The unfavorable biologic subtypes found commonly among African women include high grade tumor, estrogen receptor negative, and triple negative variety [7]. These biologic subtypes commonly present at younger age, more aggressive, and with poor prognosis. With rising prevalence of breast cancer, the burden of management of the disease in a resource-deficient economy is quite challenging [12]. The aim of this study is to report the challenges and outcome in the management of breast cancer in our setting, and thus generate data to direct our cancer policy.
MATERIALS AND METHODS
Study design
This was a prospective study conducted at Federal Teaching Hospital, Abakaliki South East Nigeria between January 2014 and April 2016. All patients presenting with breast mass with clinical diagnosis of malignancy were recruited into the study. Only patients with histological diagnosis of breast cancer were included in the analysis.
Clinical and pathologic diagnosis
A detailed pro forma-based history was taken and a thorough physical examination including the examination of the breasts was done. Ultrasound scan of the breast was done by physician radiologist when indicated.
All patients, except those with ulcerated (fungating) breast tumor, had tru-cut biopsy under local anesthesia in our surgical outpatient clinic, for histology. Those with ulcerated breast lesions had wedge biopsy under local anesthesia. All pathological reports were by consultant pathologist.
All patients had plain chest radiograph and abdominal ultrasound scan done and reported by consultant radiologist, as part of initial staging investigations. Patients with bone pain suggestive of metastases had limited skeletal survey with digital plain X-ray tomograms.
Treatment methods
Of the 18 patients who had early breast cancer, 16 had modified radical mastectomy; 2 had wide local excision (breast conservation surgery) and radiotherapy. All had adjuvant chemotherapy. Tamoxifen was prescribed routinely to all patients except in few cases when immunotyping was done and showed estrogen and progesterone receptor negative status.
All patients with locally advanced breast cancer had neoadjuvant chemotherapy followed by appropriate surgery when possible. Cyclical combination of Doxorubicin and Cyclophosphamide was given three weekly for four cycles as the main neoadjuvant protocol, except when contraindicated by abnormal electrocardiogram (ECG) and echocardiography. Docetaxel or Paclitaxel was given as second line drug to most of our patients as adjuvant chemotherapy, followed by referral for radiotherapy. However, majority of our patients were not able to travel to the distant center for radiotherapy, on grounds of lack of funds.
Treatment of recurrent breast cancer was mainly reexcision and/or chemotherapy (usually oral Capecitabine) and hormonal therapy, in the absence of radiotherapy.
Metastatic disease was treated primarily with chemotherapy and palliative care for pulmonary, bone, brain, and liver involvement. This was multidisciplinary in approach involving the general surgeons, oncologist, cardiothoracic, and orthopedic surgeons.
RESULTS
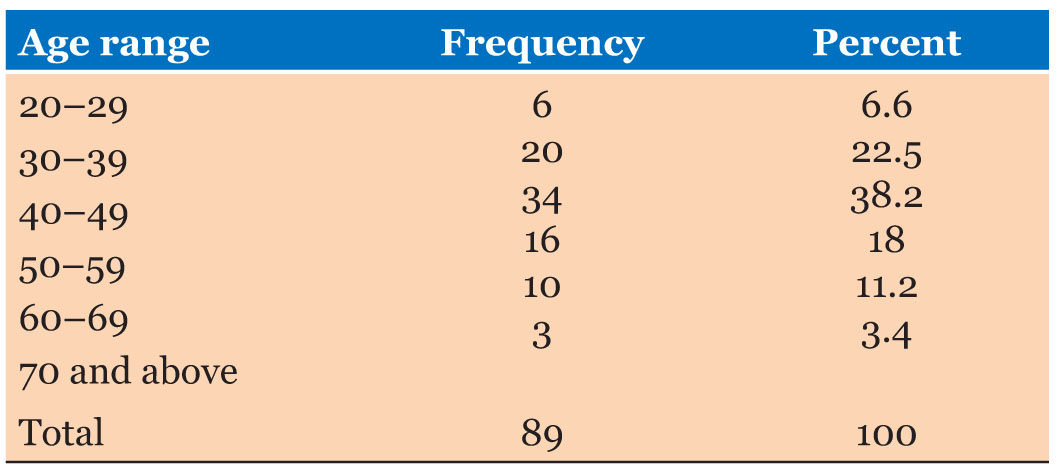
A total of 89 patients were studied. Among them two were males, giving a female to male ratio of 43.5 to 1. The mean age was 45.8 (±11.7) years; the youngest patient was 23 years. Six (6.6%) were below 30 years. Majority (60.7%) of patients were below 50 years. Only three (3.4%) were over 70 years (Table 1).
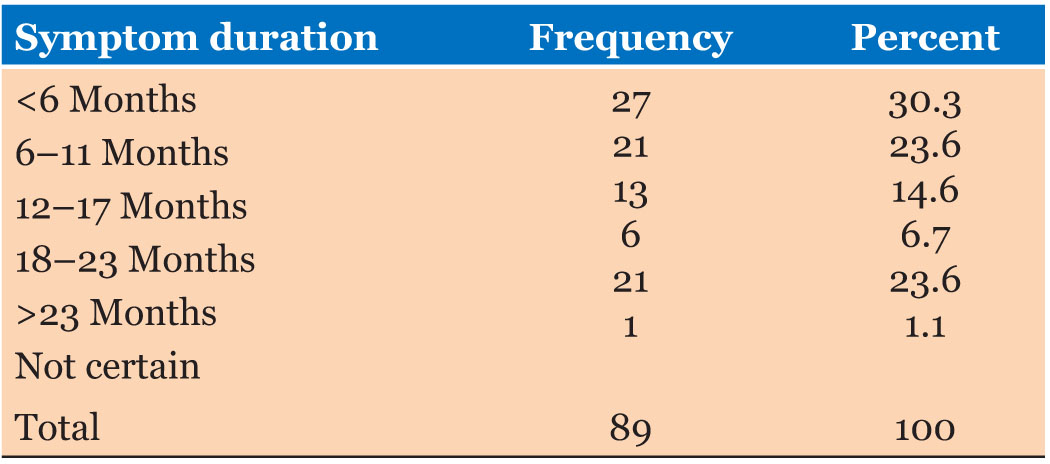
Farmers constituted the greatest number at 33 (37.1%), followed by traders and teachers with 17 (19.1%) each. Patients with only primary education or no formal education at all were 47 (52.8%). Nine patients (10.1%) admitted to consumption of alcoholic beverages; only two (2.2%) used tobacco. Twenty-seven (30.3%) patients presented to hospital within six months of their symptoms. Symptom duration before presentation was over 23 months in 21 (23.6%) patients (Table 2).
Breast mass was present in all cases (98.9%) except one; one patient with Paget’s disease of the breast presented with nipple ulceration but no palpable breast mass. In all, ulceration was a feature in 30 (33.7%). Twenty-three (25.8%) had breast pain; nipple discharge was present in six (6.7%) patients. All but one breast fed their children for over one year among 76 (85.4%) parous women. There was a family history of breast cancer in 11 (12.4%) patients; 18 (20.2%) patients used contraceptive pills. Fifty patients (56.2%) were premenopausal. The left breast had more disease alone 46 (51.7%) compared to right breast alone 39 (43.8%); there was bilateral disease in 4 (4.5%). The upper lateral quadrant had most disease 35 (39.3%); followed by central mass 21 (23.6%); mass was multiple in 19 (21.3%).
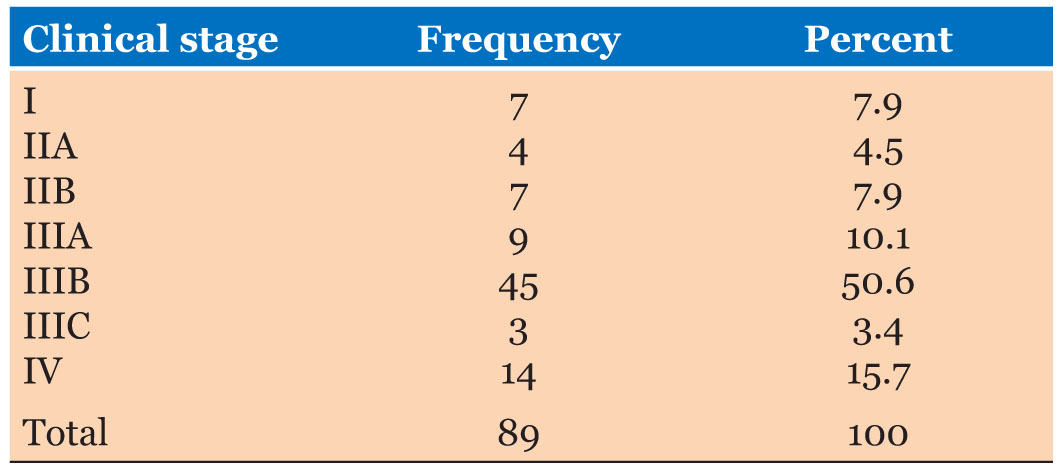
Of all only 18 (20.2%) were early disease (Stages I, IIA, and IIB); the rest 71 (79.8%) were advanced disease; 57 (64%) patients were locally advanced (Stages IIIA, B, and C). Fourteen (15.7%) were metastatic (Stage IV) disease (Table 3). The common sites of metastases were lung parenchyma (10), lungs with plural effusion (8), bone (6), spine with paralysis (2), liver (2), and brain (2). Most of the patients with metastatic disease presented with multiple metastatic sites commonly involving the lungs and widespread painful osteolytic bone lesions.
A total of 63 (70.8%) patients received neoadjuvant chemotherapy. Of these 5 (5.6%) had complete response (disappearance of all palpable lesion), 24 (27%) had partial response (≥50% reduction in size), 32 had no response (reduction in size of mass <50%), and 2 had progressive disease. However, chemotherapy interruption was common due to poor compliance. Of all the cases with advanced disease that required radiotherapy, only four patients were able to get the treatment at distant centers. Eleven of the patients (12.4%) died of advanced disease during ward admission. Of these seven deaths were from complications arising from pulmonary metastases, two from cerebral metastases, one from acute hepatic dilatation following adjuvant chemotherapy with Docetaxel, and one from intractable heart failure following neoadjuvant chemotherapy with Doxorubicin and Cyclophosphamide. Fifty-nine (66.3%) patients were lost to follow-up and are presumed dead from advanced disease. Twenty-three (25.8%) patients of this cohort remain under adjuvant therapy and follow up 2–5 years after initial diagnosis.
DISCUSSION
Our patients with breast cancer were relatively young with peak age range of 40–49 years; median age was 45 years (Table 1). This is similar to other reports from Nigeria and Africa, in contrast to the observed older age of incidence in the western world [7],[13].
However, Bowen et al. reported the median age at presentation for black women in the United Kingdom to be similar to African women at 46 years compared to 67 years in white British women [14]. Also African-American women have been noted to have a significantly younger age of incidence, compared to their Caucasian counterparts [15]. This consistent presentation of breast cancer at a younger age in the black women irrespective of environment will therefore suggest a genetic factor yet to be fully elucidated. The affectation of this younger age (working class) of women and its multiple economic ripple effects often constitute a challenge to their management in our poor resource setting.
The majority of our patients were premenopausal (56.2%). The difference in the epidemiology of breast cancer among races is also thought to be attributable to endogenous hormones. This is supported by the finding by Pinheiro et al. that premenopausal African-American women have a significantly higher level of estradiol (both absolute and free estradiol fraction) in comparison to Caucasian women [16]. Also Haiman et al. in their study noted that African-American women had higher levels of follicular and luteal phase estradiol than Caucasian women [17]. Hence breast cancer presentation during pregnancy is common in our practice, with its peculiar challenges.
Diagnosis of breast cancer is always confirmed by histology in our practice. The unavailability of routine immunohistochemistry staining for biologic subtyping of breast cancer in our setting is a major challenge. The relevance of immunotyping of breast cancer cannot be over emphasized as it is not only of prognostic value, but also helps direct adjuvant therapy for optimum outcome [18],[19]. Only 12 of our patients had immunotyping done over the period under review. Further data are therefore needed for objective analysis of the biologic profile of breast cancer in our practice. However, in their study at Jos, Northern Nigeria, Gucas et al. reported that only 25% and 27.8% of cases expressed estrogen receptor (ER) and progesterone receptor (PGR) respectively [7]. The predominantly ER and PGR negative tumors were significantly more likely to be of high grade with poor prognosis. The predominance of ER and PGR negative tumors is one factor which predicts a poorer prognosis for the Nigerian patients. They concluded that antiestrogen and other hormonal manipulations are less likely to be effective in Nigerian patients, contributing to poor outcome.
Only 20.2% of our patients presented with early breast cancer (Table 3). This is similar to report by others [7],[20]. This is partly because there is as yet no national screening program for breast cancer in Nigeria. The reverse is the case in Western Europe and America where early breast cancer constitutes over 80% and mostly detected at screening [21],[22].
Management of early breast cancer poses a special problem in our setting as most patients with early breast cancer are usually reluctant to consent for mastectomy. Yet, breast conservation surgery which is the current trend cannot be widely practiced as we do not have facility for radiotherapy. Postoperative radiotherapy after breast conserving surgery for early breast cancer is needful for improved locoregional control of the disease, with overall survival advantage [23]. Modified radical mastectomy therefore remains the main stay of surgery for early breast cancer in our practice, in spite of the psychological benefits of breast conservation surgery. Only two of our patients with early breast cancer had breast conserving surgery done and received radiotherapy from another center.
That said, the bane of breast cancer in our setting is late presentation with advanced disease. Only 30.3% of our patients presented to hospital within six months of their symptoms. Most patients try self-medication with traditional medicaments to no avail before coming to hospital. Such native medications often include herbs taken orally and or applied topically. Some patients attribute their late presentation to lack of awareness of the disease, while others attribute their late presentation to lack of funds to attend hospital. Presently, direct user charges for publicly provided health care apply to most of the population in Abakaliki, as with the rest of Nigeria. Our experience shows that fees tend to dissuade the poor natives from seeking appropriate orthodox health care services considered expensive. Hence many resort to prayer houses or ineffective native medications.
Majority of our patients had little or no education and are poor farmers. Therefore public education and improvement of socioeconomic condition of the populace may help to reduce the incidence of late presentation in our setting.
Presentation of advanced breast cancer with fungation was common, seen in 33.7% of our patients (Figure 1, Figure 2, Figure 3). This was usually due to skin invasion and spontaneous ulceration, or due to native scarifications with unsterile instrument and application of contaminated materials. Interventions by the unqualified natives in our communities tend to cause more challenging complications including ulceration, wound infection, and tetanus. One of our patients presented with tetanus from such infected wounds. Tetanus prophylaxis is necessary when the patient presents with fungation. Legislation regulating the practices of quacks are, therefore, urgently needful in Nigeria.
Most of our patients (79.8%) presented with advanced breast cancer. Advanced breast cancer is associated with poor prognosis with regard to morbidity and mortality. Peculiar challenges are encountered in the management of advanced breast in our setting. Many patients with advanced disease present with huge breast masses, sometimes involving the entire breast and the skin, plus extensive fixed axillary nodes. Majority (65.2%) of the patients had locally advanced disease (Stage III). Locally advanced breast cancer was essentially treated with neoadjuvant chemotherapy in our setting followed by appropriate surgery. For completeness of therapy, radiotherapy is necessary adjuvant in locally advanced breast cancer, as it reduces the incidence of recurrence. However, only few could access needful adjuvant radiotherapy in faraway centers in the South West or Northern Nigeria, as there was no functional radiotherapy facility in the whole of South East of Nigeria during the study period. Therefore local recurrence was common among our patients, with its attendant burden of morbidity and mortality.
Metastatic breast cancer is also common presentation in our practice. It accounted for 15.7% in this study group (Table 3). This figure is much lower than the 52.5% rate of metastatic breast cancer in a study by Adisa et al. at Ife, Western Nigeria [12]. Our staging investigations were restricted to chest X-ray to assess for pulmonary metastases, abdominal ultrasonography to assess for liver metastases, and limited skeletal survey with X-ray tomograms for any bone metastases. In the absence of facility for bone scan, some of our patients may have been under staged, accounting for the lower rate of metastatic disease in this study. Metastatic disease is often associated with severe morbidity and constitutes a heavy burden on our health care delivery system.
Eleven (12.4%) patients died on the ward, while another 59 (66.3%) were lost to follow-up and are presumed dead from advanced disease. Many of these patients prefer to die at home surrounded by close relatives. Others consider death in the hospital to be additional economic burden and tend to take their sick relative away when they view the situation to be helpless.



CONCLUSION
Breast cancer is a common presentation in our practice. Majority of our patients are young and present with advanced disease. Investigations available and treatment options for our patients are limited resulting in dismal outcome.
RECOMMENDATIONS
Health policy and budgeting should be directed at programs for early detection, adequate evaluation, and treatment of breast cancer cases. The national health insurance service of Nigeria which presently covers only a minute percentage of the populace needs to be expanded to encourage early presentation by the poor patients. Education, creation of awareness, economic empowerment of the citizenry will go a long way to reduce late presentation. Also direct government intervention including free treatment for cancer will encourage early presentation with better treatment outcome in our setting.
REFERENCES
1.
Ugwu-Olisa AO, Nnamdi ASC, Gregory NC, Festus IE. Clinicopathologic study of breast lumps in Abakaliki, South Eastern Nigeria. Asian Journal of Medical Sciences 2016;7(3):58–64. [CrossRef]

2.
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worlwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68(6):394–424. [CrossRef]
[Pubmed]
3.
Pace LE, Shulman LN. Breast cancer in Sub-Saharan Africa: Challenges and opportunities to reduce mortality. Oncologist 2016;21(6):739–44. [CrossRef]
[Pubmed]
4.
Azubuike SO, Muirhead C, Hayes L, McNally R. Rising global burden of breast cancer: The case of Sub-Saharan Africa (with emphasis on Nigeria) and implications for regional development: A review. World J Surg Oncol 2018;16(1):63. [CrossRef]
[Pubmed]
5.
Key TJ, Verkasalo PK, Banks E. Epidemiology of breast cancer. Lancet Oncol 2001;2(3):133–40. [CrossRef]
[Pubmed]
6.
DeSantis CE, Bray F, Ferlay J, Lortet-Tieulent J, Anderson BO, Jemal A. International variation in female breast cancer incidence and mortality rates. Cancer Epidemiol Biomarkers Prev 2015;24(10):1495–506. [CrossRef]
[Pubmed]
7.
Gukas ID, Jennings BA, Mandong BM, et al. Clinicopathological features and molecular markers of breast cancer in Jos, Nigeria. West Afr J Med 2005;24(3):209–13. [CrossRef]
[Pubmed]
8.
Amin SM, Ewunonu HAS, Oguntebi E, Liman IM. Breast cancer mortality in a resource-poor country: A 10 year experience in a tertiary institution. Sahel Med J 2017;20(3):93–7. [CrossRef]
9.
Gwyn K, Bondy ML, Cohen DS, et al. Racial differences in diagnosis, treatment, and clinical delays in a population-based study of patients with newly diagnosed breast carcinoma. Cancer 2004;100(8):1595–604. [CrossRef]
[Pubmed]
10.
Okobia MN, Osime U. Clinicopathological study of carcinoma of the breast in Benin City. Afr J Reprod Health 2001;5(2):56–62.
[Pubmed]
11.
Anyanwu SN. Breast cancer in eastern Nigeria: A ten year review. West Afr J Med 2000;19(2):120–5.
[Pubmed]
12.
Adisa AO, Arowolo OA, Akinkuolie AA, et al. Metastatic breast cancer in a Nigerian tertiary hospital. Afr Health Sci 2011;11(2):279–84.
[Pubmed]
13.
Ohene-Yeboah, Adjei E. Breast cancer in Kumasi, Ghana. Ghana Med J 2012;46(1):8–13.
[Pubmed]
14.
Bowen RL, Duffy SW, Ryan DA, Hart IR, Jones JL. Early onset of breast cancer in a group of British black women. Br J Cancer 2008;98(2):277–81. [CrossRef]
[Pubmed]
15.
Elmore JG, Moceri VM, Carter D, Larson EB. Breast carcinoma tumor characteristics in black and white women. Cancer 1998;83(12):2509–15. [CrossRef]
[Pubmed]
16.
Pinheiro SP, Holmes MD, Pollak MN, Barbieri LR, Hankinson SE. Racial differences in premenopausal endogenous hormones. Cancer Epidemiol Biomarkers Prev 2005;14(9):2147–53. [CrossRef]
[Pubmed]
17.
Haiman CA, Pike MC, Bernstein L, et al. Ethnic differences in ovulatory function in nulliparous women. Br J Cancer 2002;86(3):367–71. [CrossRef]
[Pubmed]
18.
Yersal O, Barutca S. Biologic subtypes of breast cancer: Prognostic and therapeutic implications. World J Clin Oncol 2014;5(3):412–24. [CrossRef]
[Pubmed]
19.
Ignatov A, Eggermann H, Burger E, Ignatov T. Patterns of breast cancer relapse in accordance to biological subtype. J Cancer Res Clin Oncol 2018;144(7):1347–55. [CrossRef]
[Pubmed]
20.
Adesunkanmi AR, Lawal OO, Adelusola KA, Durosimi MA. The severity, outcome and challenges of breast cancer in Nigeria. Breast 2006;15(3):399–409. [CrossRef]
[Pubmed]
21.
McPhail S, Johnson S, Greenberg D, Peake M, Rous B. Stage at diagnosis and early mortality from cancer in England. Br J Cancer 2015;112 Suppl 1:S108–15. [CrossRef]
[Pubmed]
22.
American Cancer Society. Breast Cancer: Facts & Figures 2017–2018. Atlanta: American Cancer Society, Inc.; 2017.
23.
Speers C, Pierce LJ. Postoperative radiotherapy after breast-conserving surgery for early-stage breast cancer: A review. JAMA Oncol 2016;2(8):1075–82. [CrossRef]
[Pubmed]
SUPPORTING INFORMATION
Acknowledgments
The authors wish to acknowledge the priceless contribution of the surgical residents who helped with the completion of the study pro forma.
Author ContributionsUche Emmanuel Eni - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Uchenna Chinedu Dilibe - Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ogbuanya Aloysius Ugwu - Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Umezurike Harold Akuma Daniel - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Otuu Onyeyirichi - Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Oji Uzor Ekuma - Conception of the work, Design of the work, Acquisition of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2019 Uche Emmanuel Eni et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.


